Most people have a pretty clear mental image of acid reflux. Burning in the chest after a meal. A sour taste rising into the throat. The classic heartburn that sends you reaching for a Tums at 10pm. It is uncomfortable, it is recognizable, and it tells you pretty directly that something is going wrong in your digestive tract.
But there is another form of acid reflux that works very differently. It does not cause the chest burning most people associate with GERD. It does not produce the obvious sour taste or the retrosternal discomfort that sends people to the pharmacy. Instead it shows up as a chronic cough that will not go away no matter how many times you treat it for allergies. A hoarse voice in the morning that improves through the day. The persistent feeling of something stuck in your throat. A need to clear your throat constantly, often in situations where it feels socially awkward to do so.
This is laryngopharyngeal reflux, almost always referred to as LPR, and it is frequently called silent reflux precisely because it can cause significant, ongoing damage to the throat and airway without ever producing the heartburn that most people use to recognize acid reflux in the first place.
LPR is underdiagnosed, frequently misattributed to allergies or post-nasal drip or chronic sinusitis, and poorly understood by many people who have been living with its symptoms for years. This article explains exactly what it is, why it feels so different from typical GERD, how it is diagnosed, and what the evidence says about managing it effectively.
This is the final article in our GERD series. For the complete foundation on acid reflux and GERD, visit our GERD and Acid Reflux Explained guide.
What LPR Actually Is
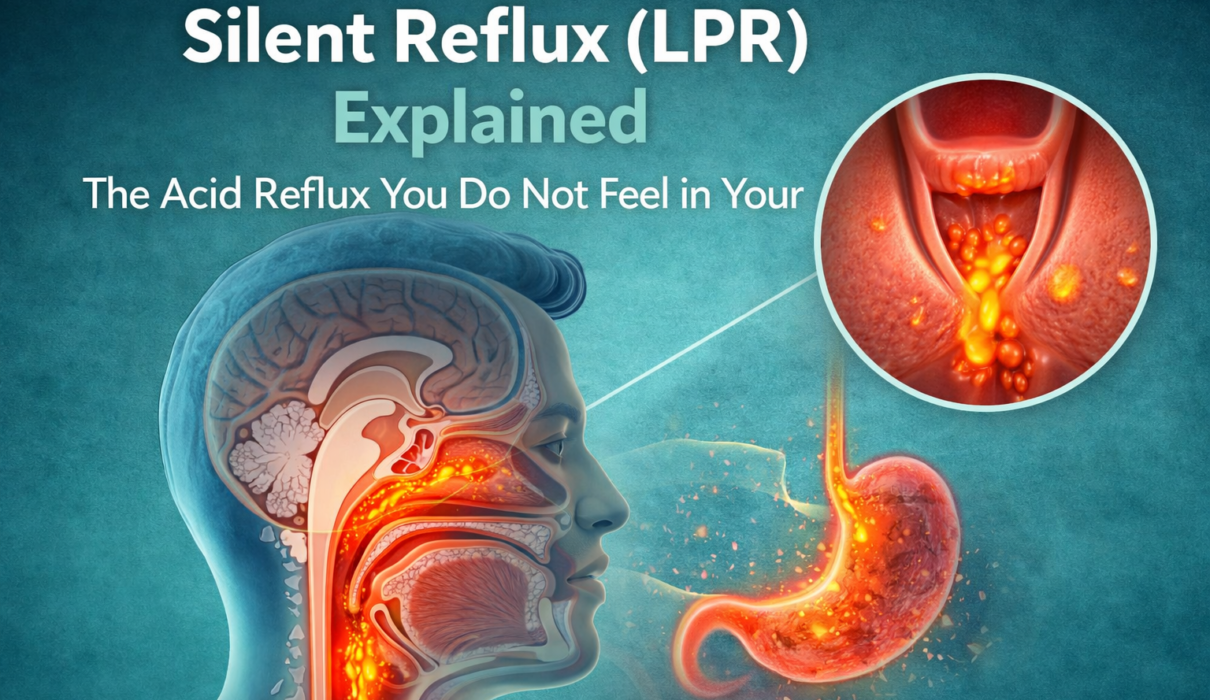
Laryngopharyngeal reflux is a condition in which stomach contents, including acid and in some cases digestive enzymes like pepsin, travel upward past the upper esophageal sphincter and reach the larynx, pharynx, and sometimes even the airway and nasal passages.
To understand why this is different from typical GERD, a brief anatomy refresher helps.
In standard GERD, the lower esophageal sphincter fails to keep stomach contents from entering the esophagus. The esophagus gets exposed to acid, which causes the familiar heartburn sensation and, over time, esophageal inflammation and damage.
In LPR, the reflux goes further. It travels up the entire length of the esophagus and gets past the upper esophageal sphincter, which is the second valve at the top of the esophagus where it meets the throat. When stomach contents reach this level, they come into contact with the larynx, the structure containing the vocal cords, and the pharynx, the back of the throat. These tissues are exquisitely sensitive to acid and have virtually none of the acid-tolerance that the esophagus develops through repeated exposure (Koufman, 1991).
This extreme sensitivity is precisely why such small amounts of reflux in LPR can cause such significant symptoms. The larynx can be irritated by brief, infrequent acid contact that would barely register in the esophagus. A person with LPR can have just a few reflux episodes per day, far fewer than a typical GERD patient, and still develop chronic hoarseness, throat irritation, and airway symptoms from those small exposures.
Why LPR Does Not Cause Heartburn
This is the question that confuses most people, including some healthcare providers, when LPR first comes up. If acid is refluxing, why does it not burn?
The answer has to do with contact time and location.
In GERD, acid sits in the esophagus for extended periods, repeatedly bathing the same tissue and generating the sustained burning sensation most people recognize as heartburn. The esophageal lining, while not designed for acid exposure, is at least more tolerant of it than the throat structures are.
In LPR, the acid often passes through the esophagus relatively quickly without causing significant esophageal symptoms. It reaches the throat, causes irritation there, and then the esophagus clears. The contact time in the esophagus is too brief in many LPR cases to trigger the classic heartburn response, but the throat and larynx are sensitive enough that even that brief exposure at the upper end causes problems.
This is why research estimates that up to 50 percent of people with LPR do not experience classic heartburn (Koufman et al., 2002). The absence of heartburn does not mean the absence of reflux. It means the reflux is predominantly affecting a different location.
Recognizing LPR: The Symptoms Most People Miss
Because LPR does not present the way most people expect acid reflux to present, its symptoms are routinely attributed to other conditions. Understanding the specific symptom pattern of LPR is the first step toward getting it correctly identified.
Chronic Throat Clearing
This is one of the most common and most characteristic symptoms of LPR. People with LPR often feel a persistent need to clear their throat, not because of mucus from a cold or allergy but because of irritation and inflammation in the laryngopharyngeal area from acid exposure. The throat clearing itself can further irritate the already-inflamed tissues, creating a frustrating cycle.
Hoarseness and Voice Changes
Acid reaching the larynx irritates the vocal cords, causing hoarseness, vocal fatigue, or a change in voice quality. This is often most noticeable in the morning because overnight reflux, when the body is horizontal and swallowing frequency drops, allows acid to reach the throat and sit there. Many people with LPR notice their voice is rough or strained when they first wake up and gradually improves through the day as swallowing and saliva production help clear the irritation.
Chronic Cough
A persistent cough is one of the most common reasons people see their doctor and one of the conditions most frequently linked to LPR when other obvious causes have been ruled out. The cough in LPR is typically dry, often worse at night or in the early morning, and does not respond to standard cough treatments or antihistamines the way an allergy or post-nasal drip cough would.
Globus Sensation
Globus is the medical term for the feeling that something is stuck in the throat, often described as a lump sensation, tightness, or the feeling that there is a pill that never quite went down. It is not painful and does not actually interfere with swallowing, but it is persistent and often distressing. Globus is one of the classic symptoms of LPR and is caused by inflammation and swelling of the laryngopharyngeal tissues from repeated acid exposure (Moloy and Charter, 1982).
Excess Throat Mucus or Post-Nasal Drip Sensation
Many people with LPR describe what feels like post-nasal drip, a sensation of mucus draining from the back of the nose into the throat. In many of these cases, the mucus sensation is not actually coming from the sinuses but is instead the throat producing excess mucus in response to acid irritation, a protective response that can feel identical to true post-nasal drip.
Difficulty Swallowing
Mild difficulty swallowing, particularly a sensation that food moves slowly or catches slightly in the throat, can occur in LPR due to inflammation and swelling of the pharyngeal tissues. Significant or progressive difficulty swallowing always warrants prompt medical evaluation regardless of the suspected cause.
Worsening Asthma or Reactive Airway Symptoms
Acid reaching the airway can trigger bronchospasm and worsen asthma symptoms. People with poorly controlled asthma, particularly nighttime or early morning symptoms, should have LPR considered as a potential contributing factor, especially when standard asthma management is not providing adequate control.
How LPR Is Diagnosed
Diagnosing LPR is more complex than diagnosing typical GERD, and this complexity is part of why it is so frequently missed or misattributed.
Standard GERD testing is not always helpful for LPR. A regular upper endoscopy may show a completely normal esophagus in someone with significant LPR because the damage in LPR is occurring primarily in the throat and larynx rather than the esophagus. A normal endoscopy does not rule out LPR.
The most direct diagnostic approach is laryngoscopy, a procedure in which an ear, nose, and throat specialist, called an ENT or otolaryngologist in the United States, uses a thin flexible scope to directly visualize the larynx and vocal cords. In people with LPR, characteristic findings include redness and swelling of the arytenoids (small cartilages at the back of the larynx), thickening and swelling of the posterior laryngeal area, and sometimes nodules or other changes to the vocal cords from chronic irritation (Belafsky et al., 2001).
A validated clinical tool called the Reflux Symptom Index, or RSI, is a nine-question questionnaire that helps quantify LPR symptom burden and is widely used by ENT providers in the United States to assess and track LPR patients. An RSI score above 13 is considered suggestive of LPR.
pH monitoring, either through a traditional catheter-based 24-hour study or a wireless pH capsule (the Bravo pH capsule system), can measure acid exposure at multiple levels of the esophagus, including the upper esophagus. Impedance-pH testing, which detects both acidic and non-acidic reflux events, is considered the most comprehensive diagnostic study for suspected LPR.
In many American clinical settings, particularly in primary care and ENT practice, LPR is diagnosed empirically based on the clinical symptom pattern and laryngoscopic findings, with formal pH testing reserved for cases where the diagnosis is unclear or where treatment is not producing the expected response.
The Role of Pepsin in LPR
One of the most interesting and clinically relevant aspects of LPR that distinguishes it from standard acid reflux is the role of pepsin, a digestive enzyme produced by the stomach.
Pepsin is active in an acidic environment and is designed to break down proteins during digestion. When pepsin is carried upward in refluxate and reaches the laryngeal tissues, it can remain embedded in those tissues even after the acid itself has been neutralized or cleared. In this embedded state, pepsin can be reactivated by any local acidity, including acidic foods or beverages, and continue to cause tissue damage (Johnston et al., 2007).
This has important implications for management. It helps explain why some people with LPR find that acidic foods and drinks, including citrus juice, soda, coffee, and wine, worsen their throat symptoms significantly even when the overall acid level in their esophagus appears normal. The pepsin already present in the throat tissue is being reactivated by the local acidity of these foods, not by a new reflux event.
It also explains why LPR can sometimes be more difficult to treat than typical GERD and why acid suppression alone, while helpful, may not fully resolve symptoms in all patients.
Managing LPR: What Actually Works
Managing LPR requires a somewhat different approach than managing typical GERD. The treatments overlap significantly but the emphasis differs, and the timeline for improvement is longer than most patients expect.
Dietary Modifications
Diet plays a particularly important role in LPR management because of the pepsin reactivation mechanism described above. Beyond the standard GERD trigger foods, people with LPR are often advised to pay specific attention to dietary acidity.
A low-acid diet, in which foods and beverages with a pH below 4 or 5 are minimized or avoided, has shown benefit in LPR management in several studies. This specifically targets the pepsin reactivation pathway by reducing the local acidity that wakes up embedded pepsin in the throat tissues (Koufman and Johnston, 2012).
Carbonated beverages are particularly problematic in LPR because they are both acidic and introduce gas that promotes reflux events. Even sparkling water, which is marketed as a healthier alternative to soda, is acidic enough to potentially reactivate pepsin and worsen LPR symptoms.
Coffee, citrus juices, tomato products, wine, and most sodas all fall below a pH of 4 and are worth reducing or eliminating during an initial treatment period to assess their contribution to symptoms.
Eating Behaviors and Timing
The same behavioral principles that apply to GERD apply in LPR, often with even more emphasis. Eating at least three hours before lying down, keeping portions moderate, eating slowly, and avoiding eating close to bedtime are all important.
Because overnight reflux is particularly damaging in LPR due to the reduced swallowing and saliva production during sleep, the pre-bedtime eating window is one of the highest-leverage behavioral changes available.
Elevating the Head of the Bed
Proper head of bed elevation, six to eight inches using bed risers or a wedge under the mattress rather than extra pillows, reduces overnight acid exposure reaching the throat. This is particularly relevant in LPR where nighttime reflux causes throat and laryngeal symptoms that are most prominent in the morning.
Proton Pump Inhibitors
PPIs are the primary pharmacological treatment for LPR, but the treatment approach differs from standard GERD in two important ways.
First, twice-daily PPI dosing, one dose 30 to 60 minutes before breakfast and one dose 30 to 60 minutes before dinner, is typically recommended for LPR rather than the once-daily dosing that is often sufficient for typical GERD. This is because more complete acid suppression throughout the day is needed to reduce the frequency and acidity of reflux reaching the sensitive laryngeal tissues.
Second, the treatment timeline is significantly longer. While typical GERD symptoms often improve within two to four weeks of starting a PPI, LPR symptoms frequently take two to three months of consistent treatment to show meaningful improvement, and some patients require four to six months before significant relief is achieved (Reichel et al., 2008). This extended timeline is one of the most common reasons LPR treatment fails, as patients or providers conclude the treatment is not working and stop it prematurely.
It is important to note that PPIs do not address the non-acid components of reflux, including the pepsin discussed above. This is why dietary modification is considered an important complement to PPI therapy in LPR rather than an optional add-on.
Alginates
Sodium alginate preparations, available in the United States as products like Gaviscon Advance (the formulation available in the US differs from the UK version), work by forming a physical raft on top of stomach contents that helps prevent reflux from reaching the esophagus and throat. They are increasingly used as an adjunct to PPI therapy in LPR management, particularly for post-meal and nighttime symptoms, and some research suggests they may be particularly helpful for LPR given their mechanical barrier effect on the refluxate that carries pepsin (McGlashan et al., 2009).
Voice Therapy
For people with significant voice changes, hoarseness, or vocal fatigue from LPR, working with a speech-language pathologist who specializes in voice disorders can be a valuable part of the treatment approach. Voice therapy does not treat the reflux itself but helps rehabilitate the vocal cords and teaches techniques to reduce the additional strain that throat clearing and compensatory voice behaviors place on already-irritated tissues.
LPR vs GERD: Key Differences at a Glance
People often wonder whether they have LPR, GERD, or both. The two conditions can coexist, and many people with chronic GERD also have some degree of laryngopharyngeal involvement. But the distinctions in where symptoms occur, what they feel like, and how they respond to treatment are meaningful enough to be worth summarizing clearly.
In GERD, the primary symptoms are heartburn, regurgitation, and chest discomfort. The damage occurs in the esophagus. Standard once-daily PPI dosing is usually effective, and symptom improvement is typically seen within weeks.
In LPR, the primary symptoms are throat clearing, hoarseness, chronic cough, and globus sensation. Heartburn is often absent. The damage occurs in the larynx and pharynx. Twice-daily PPI dosing is typically required, dietary acidity is a specific concern due to pepsin, and treatment response takes months rather than weeks.
Understanding which condition you are dealing with, or whether both are present, significantly affects how management should be approached and what timeline for improvement is realistic to expect.
Frequently Asked Questions
Q: I have had a chronic cough for over a year that my doctor keeps treating as allergies. Could it be LPR? Possibly, especially if antihistamines and allergy treatments have not provided meaningful relief, if the cough is dry rather than productive, and if it is worse in the morning or after meals. LPR is one of the three most common causes of chronic cough in adults along with upper airway cough syndrome and asthma. Asking your doctor for a referral to an ENT for laryngoscopy is a reasonable next step if LPR has not been considered.
Q: Can LPR damage my vocal cords permanently? Chronic, unmanaged LPR can cause persistent changes to the vocal cords and laryngeal tissues including thickening, granulomas, and nodules. With appropriate treatment and management, these changes typically resolve over time. Longstanding untreated LPR carries more risk of persistent changes, which is one reason getting an accurate diagnosis and starting effective management sooner rather than later matters.
Q: Why does my throat feel worse in the morning even though I do not eat at night? Overnight reflux is a primary driver of LPR morning symptoms. When you are lying down and swallowing frequency drops, small amounts of reflux can reach the throat and sit there for extended periods without being cleared. Elevating the head of the bed and avoiding eating for at least three hours before bed are the most effective behavioral interventions for morning throat symptoms specifically.
Q: My ENT diagnosed me with LPR but my gastroenterologist says my acid levels are normal. Who is right? Both can be correct simultaneously. LPR often involves very small amounts of reflux that do not register as abnormal on standard esophageal acid testing, but are still sufficient to irritate the highly sensitive laryngeal tissues. The diagnosis of LPR is primarily clinical and laryngoscopic. Normal esophageal pH testing does not rule it out.
Q: How long will I need to take a PPI for LPR? This varies by individual and by the severity of the condition. Most guidelines recommend a minimum treatment trial of two to three months with twice-daily dosing before assessing response. Some people require longer courses. The goal after achieving symptom control is generally to step down to the lowest effective dose while maintaining the lifestyle and dietary modifications that reduce reflux frequency.
This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for personal health concerns.
References
Koufman JA. The otolaryngologic manifestations of gastroesophageal reflux disease: a clinical investigation of 225 patients using ambulatory 24-hour pH monitoring and an experimental investigation of the role of acid and pepsin in the development of laryngeal injury. Laryngoscope. 1991;101(4 Pt 2 Suppl 53):1–78. https://pubmed.ncbi.nlm.nih.gov/2023310
Koufman JA, Aviv JE, Casiano RR, Shaw GY. Laryngopharyngeal reflux: position statement of the committee on speech, voice, and swallowing disorders of the American Academy of Otolaryngology-Head and Neck Surgery. Otolaryngol Head Neck Surg. 2002;127(1):32–35. https://pubmed.ncbi.nlm.nih.gov/12161727
Belafsky PC, Postma GN, Koufman JA. Validity and reliability of the reflux symptom index. J Voice. 2002;16(2):274–277. https://pubmed.ncbi.nlm.nih.gov/12150380
Johnston N, Knight J, Dettmar PW, Lively MO, Koufman J. Pepsin and carbonic anhydrase isoenzyme III as diagnostic markers for laryngopharyngeal reflux disease. Laryngoscope. 2004;114(12):2129–2134. https://pubmed.ncbi.nlm.nih.gov/15564833
Koufman JA, Johnston N. Potential benefits of pH 8.8 alkaline drinking water as an adjunct in the treatment of reflux disease. Ann Otol Rhinol Laryngol. 2012;121(7):431–434. https://pubmed.ncbi.nlm.nih.gov/22844861
Reichel O, Dressel H, Wiederanders K, Issing WJ. Double-blind, placebo-controlled trial with esomeprazole for symptoms and signs associated with laryngopharyngeal reflux. Otolaryngol Head Neck Surg. 2008;139(3):414–420. https://pubmed.ncbi.nlm.nih.gov/18722224
McGlashan JA, Johnstone LM, Sykes J, Strugala V, Dettmar PW. The value of a liquid alginate suspension (Gaviscon Advance) in the management of laryngopharyngeal reflux. Eur Arch Otorhinolaryngol. 2009;266(2):243–251. https://pubmed.ncbi.nlm.nih.gov/18629531
Moloy PJ, Charter R. The globus symptom: incidence, therapeutic response, and age and sex relationships. Arch Otolaryngol. 1982;108(11):740–744. https://pubmed.ncbi.nlm.nih.gov/7138257