
If you have ever read anything about acid reflux or GERD, you have probably come across the term lower esophageal sphincter, usually abbreviated as LES. It gets mentioned briefly, described as a valve that is not working properly, and then the article moves on to talk about symptoms and treatments.
What rarely gets explained is what this valve actually is, how it works when it is functioning correctly, why it fails, and what that failure means for your body over time. That gap in understanding matters, because the LES is not just a minor mechanical detail. It is the central structure around which the entire physiology of acid reflux revolves.
Understanding how it works gives you a far clearer picture of why certain foods worsen reflux, why position matters, why some medications work the way they do, and why GERD is fundamentally a structural problem rather than simply a matter of producing too much acid.
This article fills that gap. No shortcuts, no oversimplification. Just a clear explanation of one of the most important and least understood structures in digestive health.
This article is part of our GERD series. If you are looking for the full picture of acid reflux and GERD, start with our GERD and Acid Reflux Explained guide.
What the Lower Esophageal Sphincter Actually Is
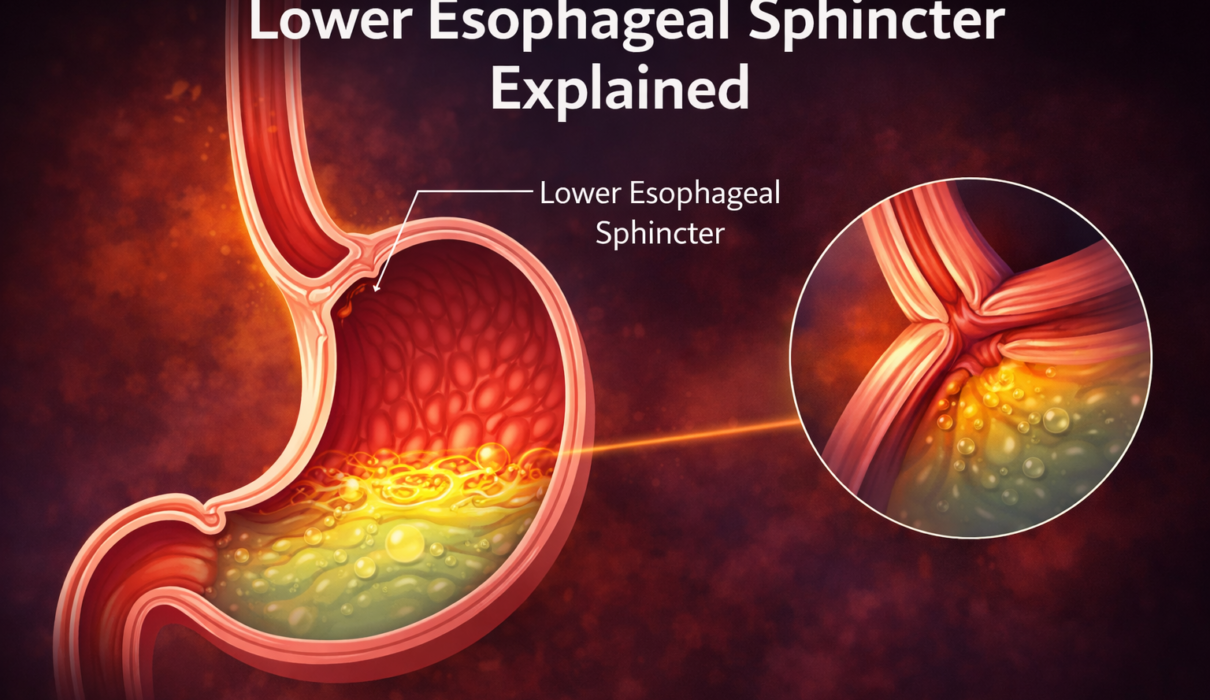
The lower esophageal sphincter is a ring of smooth muscle located at the junction between the esophagus and the stomach, roughly at the level of the diaphragm. It is not a discrete anatomical structure in the way a valve in a machine is. There is no visible flap or door. It is instead a thickened, tonically contracted segment of the circular muscle layer of the esophagus that maintains continuous pressure at that junction.
In a healthy, resting state, the LES maintains a pressure of approximately 10 to 45 mmHg above gastric pressure. This means the valve is actively closed, held shut by muscular tone, creating a high-pressure zone that prevents stomach contents from flowing backward into the esophagus (Mittal and Balaban, 1997).
Think of it less like a door and more like a hand squeezing a hose. The squeeze is constant and active. The moment the squeeze relaxes inappropriately, whatever is in the hose can travel backward.
The LES sits at the point where the esophagus passes through the diaphragm, the large dome-shaped muscle that separates the chest cavity from the abdominal cavity. The diaphragm itself contributes to the barrier function of the LES, acting as an external pinch-point that adds additional mechanical support to the muscular sphincter. This combined anatomical arrangement, the intrinsic LES tone plus the extrinsic diaphragmatic support, is what makes the junction effective under normal circumstances.
How the LES Opens and Closes
The LES does not stay closed all the time. It has two distinct and physiologically important reasons to open.
The first is swallowing. When you swallow, a coordinated wave of muscle contractions called peristalsis moves food down the esophagus toward the stomach. Immediately before the food arrives at the LES, the sphincter receives a neural signal and relaxes, opening to allow food to pass into the stomach. Once food has passed through, the LES returns to its resting contracted state within a few seconds.
The second is belching. Transient LES relaxations, or TLESRs, are brief spontaneous relaxations of the sphincter that occur independently of swallowing. Their primary physiological purpose is to allow gas to escape from the stomach upward through the esophagus, which is the mechanism behind normal belching. These transient relaxations are coordinated by the vagus nerve and are a completely normal part of gastric physiology.
The problem arises when TLESRs occur too frequently, last too long, or are accompanied by liquid stomach contents rather than just gas. In these situations, acid travels upward into the esophagus along with the gas, producing a reflux event.
Research has established that the majority of reflux events in people with GERD are caused by these transient LES relaxations rather than by a chronically weak sphincter (Dodds et al., 1982). This is an important distinction because it means that GERD in most people is not simply a matter of a sphincter that has lost all tone. It is a matter of a sphincter that relaxes too often or at the wrong times.
What Weakens or Disrupts the LES
Several factors can reduce resting LES pressure, increase the frequency of transient relaxations, or impair the sphincter’s ability to respond appropriately to increases in abdominal pressure.
Foods and Dietary Factors
Certain foods directly reduce LES pressure or promote transient relaxations. Fatty foods are among the most consistently documented, as they promote the release of cholecystokinin, a gut hormone that reduces LES tone. Chocolate, caffeine, alcohol, and peppermint all have documented effects on LES pressure through various mechanisms (Becker et al., 1989).
This is the physiological basis for why dietary modification is a genuine first-line intervention in GERD management, not just a lifestyle suggestion. You are directly influencing the pressure dynamics at the LES with what you eat and drink.
Medications
A number of commonly used medications reduce LES pressure as a side effect. These include calcium channel blockers, which are used for blood pressure and heart conditions, certain asthma medications including theophylline, benzodiazepines, progesterone-containing medications, and some antidepressants and antipsychotics (Richter, 2007).
If you are on any of these medications and experience significant reflux, it is worth discussing with your doctor whether the medication may be contributing and whether alternatives exist.
Hiatal Hernia
A hiatal hernia is one of the most clinically significant structural factors affecting LES function. It occurs when part of the stomach pushes upward through the hiatus, the opening in the diaphragm through which the esophagus passes, into the chest cavity.
This disrupts the normal anatomical arrangement in two important ways. First, it separates the intrinsic LES from the external support provided by the diaphragmatic crura, the muscular pillars that normally reinforce the sphincter from the outside. Second, when the stomach is partially above the diaphragm, a pocket forms where acid can accumulate above the diaphragm. This acid reservoir is closer to the esophagus and more easily refluxes with any LES relaxation.
Not every hiatal hernia causes symptoms, and not every person with GERD has a hiatal hernia. But the two frequently coexist, and a larger hernia is associated with more severe reflux and a higher likelihood of complications (Hyun and Bak, 2011).
Obesity and Increased Abdominal Pressure
The LES functions within a pressure environment. Its effectiveness depends on maintaining adequate pressure relative to the stomach. When intra-abdominal pressure rises, as it does with obesity, pregnancy, chronic constipation, or even tight clothing, the pressure gradient across the LES is altered. The LES must work against greater force to remain closed.
In people with significant abdominal obesity, this chronically elevated pressure is a persistent mechanical stress on the sphincter, promoting both resting reflux and increased transient relaxation frequency. This is why weight loss is one of the most effective and evidence-supported interventions for reducing GERD severity in people who are overweight (Hampel et al., 2005).
Smoking
Nicotine reduces LES pressure directly and also impairs saliva production. Saliva plays an important role in neutralizing acid in the esophagus after reflux events. The combination of a weaker sphincter and reduced natural acid clearance makes smoking a significant contributor to both reflux frequency and esophageal damage (Chattopadhyay, 2004).
Hormonal Factors
Progesterone, a hormone that rises during pregnancy, has a relaxing effect on smooth muscle throughout the body, including the LES. This is a primary reason why GERD is extremely common during pregnancy, particularly in the second and third trimesters, and typically resolves after delivery.
What Happens When the LES Fails Over Time
A single reflux event causes transient contact between stomach acid and the esophageal lining. The esophagus has some capacity to recover from brief exposures through a process involving restored blood flow, cellular repair, and continued saliva neutralization. The problem is cumulative exposure over months and years.
When the LES fails repeatedly, acid contact time in the esophagus accumulates. The esophageal lining, which unlike the stomach does not have a robust protective mucus layer, begins to show signs of damage. This presents initially as inflammation, called esophagitis, and in more significant cases as visible erosions in the mucosal lining.
With prolonged, inadequately managed acid exposure, the body adapts by replacing the normal esophageal lining cells with a different cell type better suited to an acid environment. This process is called intestinal metaplasia and is the defining feature of Barrett’s esophagus, a pre-cancerous condition that develops in a subset of people with chronic GERD.
Understanding this progression is part of why LES dysfunction is not merely an inconvenience. It is the upstream cause of a chain of events that, without adequate management, can lead to meaningful structural changes in the esophagus over time.
Can the LES Be Strengthened or Repaired
This is the question most people eventually ask, and the honest answer is nuanced.
The LES cannot be strengthened through exercise in the way skeletal muscles can be trained. It is smooth muscle, controlled by the autonomic nervous system rather than voluntary effort. You cannot do exercises to directly increase its resting tone.
What you can do is reduce the factors that weaken it. Avoiding LES-relaxing foods, stopping smoking, losing weight if indicated, reviewing medications that reduce LES pressure, and treating any contributing conditions like hiatal hernia all reduce the functional burden on the sphincter without requiring the muscle itself to change.
For people with severe, medically refractory GERD, procedural options that mechanically reinforce the LES do exist. The Nissen fundoplication wraps the upper part of the stomach around the LES to provide external structural support, effectively recreating the anatomical reinforcement that is lost in hiatal hernia or with LES laxity. The LINX device, a newer approach, places a small ring of magnetic beads around the LES that allows food to pass while resisting retrograde acid flow. Both have evidence supporting their effectiveness in appropriately selected patients (Ganz et al., 2013).
Why This Understanding Changes How You Approach GERD
Most people who are told they have GERD think of it as a stomach acid problem. And because that is the framing, they reach for antacids, which neutralize acid, or PPIs, which reduce acid production. These treatments address the consequences of LES dysfunction rather than the dysfunction itself.
That is not a criticism of those treatments. Reducing acid does reduce esophageal damage and symptom burden, and it is appropriate and effective management for many people. But it explains why GERD rarely goes away permanently with medication alone, while the underlying structural contributors remain unaddressed.
The most complete approach to GERD combines symptom and acid management with direct attention to the factors that impair LES function. Dietary choices, body weight, smoking, medication review, sleep position, and meal timing are all things that directly influence what happens at the LES, not just how much acid the stomach produces.
This is why lifestyle modification is not just an optional add-on to medical treatment. It is intervention at the level of the actual mechanism.
Frequently Asked Questions
Q: Is a weak LES the same as a hiatal hernia? No. They are related but distinct. A weak or dysfunctional LES refers to reduced sphincter tone or increased transient relaxations. A hiatal hernia is a structural displacement of part of the stomach above the diaphragm. A hiatal hernia worsens LES function by disrupting its anatomical support, but you can have LES dysfunction without a hernia, and a small hiatal hernia without significant LES dysfunction.
Q: Does everyone with GERD have a weak LES? Not necessarily in the sense of permanently reduced resting tone. Research shows that the majority of reflux events in GERD patients are caused by transient LES relaxations occurring too frequently, rather than a sphincter that has lost all baseline tone. The distinction matters because it shifts the focus toward understanding what triggers those relaxations rather than assuming the sphincter is simply broken.
Q: Can you feel the LES relaxing when reflux happens? Not directly. What you feel is the consequence of acid contacting the esophageal lining, which is the heartburn or burning sensation. The LES relaxation itself is not perceptible. This is part of why silent reflux, where acid enters the esophagus without producing obvious heartburn, is possible and clinically significant.
Q: Why does lying down make reflux worse if the LES is the problem? The LES is the primary barrier against reflux, but gravity provides important supplementary support in the upright position. When you lie down, gravity no longer helps keep stomach contents away from the LES. Even a partially dysfunctional LES that manages fine while you are upright may allow reflux events when you are horizontal and the gravitational assistance is removed.
Q: If I have surgery for GERD, does that fix the LES permanently? Surgical options like fundoplication and the LINX device provide mechanical reinforcement of the LES and have good long-term outcomes in appropriate candidates. However, they address the structural problem rather than eliminating the underlying physiological tendency toward transient relaxations. Most people see dramatic improvement, but some degree of ongoing attention to dietary and lifestyle factors remains relevant after surgery.
Practical Takeaway
The lower esophageal sphincter is the valve at the heart of acid reflux. It is a ring of smooth muscle that keeps stomach contents from traveling back into the esophagus through active muscular tone. When it relaxes too often, stays open too long, or is weakened by structural disruption, reflux occurs and the esophageal lining pays the price.
Understanding what affects LES function, including diet, body weight, smoking, medications, hiatal hernia, and hormonal factors, gives you direct insight into why the evidence-based management strategies for GERD work the way they do. They are not arbitrary recommendations. They are interventions aimed at the specific mechanisms that determine how well this valve does its job.
Final Thoughts
The lower esophageal sphincter is a small structure with an outsized role in digestive health. Most people living with GERD have never had it explained to them in terms that connect the anatomy to the symptoms, the symptoms to the damage, and the damage to the management strategies.
That connection is exactly what makes understanding it worthwhile. You are not just managing a burning sensation. You are managing the long-term health of a valve that, when it works well, you will never think about at all.
For the complete guide to GERD including causes, symptoms, diagnosis, and treatment, visit our GERD and Acid Reflux Explained guide.
Disclaimer: This article is for educational purposes only and does not constitute medical advice.
References
Mittal RK, Balaban DH. The esophagogastric junction. N Engl J Med. 1997;336(13):924–932. https://pubmed.ncbi.nlm.nih.gov/9070474
Dodds WJ, Dent J, Hogan WJ, et al. Mechanisms of gastroesophageal reflux in patients with reflux esophagitis. N Engl J Med. 1982;307(25):1547–1552. https://pubmed.ncbi.nlm.nih.gov/7144836
Becker DJ, Sinclair J, Castell DO, Wu WC. A comparison of high and low fat meals on postprandial esophageal acid exposure. Am J Gastroenterol. 1989;84(7):782–786. https://pubmed.ncbi.nlm.nih.gov/2741879
Hyun JJ, Bak YT. Clinical significance of hiatal hernia. Gut Liver. 2011;5(3):267–277. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3166665/
Hampel H, Abraham NS, El-Serag HB. Meta-analysis: obesity and the risk for gastroesophageal reflux disease and its complications. Ann Intern Med. 2005;143(3):199–211. https://pubmed.ncbi.nlm.nih.gov/16061918
Richter JE. Role of the gastric refluxate in gastroesophageal reflux disease: acid, weak acid and bile. Am J Med Sci. 2009;338(2):89–95. https://pubmed.ncbi.nlm.nih.gov/19652537
Ganz RA, Peters JH, Horgan S, et al. Esophageal sphincter device for gastroesophageal reflux disease. N Engl J Med. 2013;368(8):719–727. https://pubmed.ncbi.nlm.nih.gov/23425164
Chattopadhyay DK. Effect of smoking on the lower esophageal sphincter. Indian J Gastroenterol. 2004;23(2):73–74. https://pubmed.ncbi.nlm.nih.gov/15176969
1 Comment